
Your first personal, practical guide to avoid getting COVID (Maybe again?)
Introduction and Part 1 of 10


Exchanging aerosols. Generated by DALL-E 2.
Introduction
OMG. More about COVID? What for? Why do you need this? I promise you, this one is different and I hope will be the most practical one you have seen. I have facts, perspectives, and workable suggestions you haven’t heard. I spent my whole medical career trying to be as practical as possible and that is what I am trying to do for you here. I want some of this to surprise you, so, if you already know most of this, I have failed.
Who is this series for? If you cannot be persuaded that COVID is still a problem or that vaccines or masks are useful tools, then I am not going to convince you of much, so you can stop here. If you are still concerned about COVID for yourself, your family and friends, and have questions that haven’t been answered in the sources you read, I hope that this series is chock full of new facts and ideas for you.
Disclaimer: these are solely my own opinions (based on lots of reading, observations, experience and thinking). I am not representing or speaking for anyone else.
This is presented as a 10-part series, with all parts currently online:
Part 1: How bad is COVID, really, and what to do with the new CDC recommendations?
Part 2: Why else should we still care about COVID?
Part 3: Masks (section 1 of 2)
Part 4: Masks (Section 2 of 2)
Part 5: Aerosols, ventilation, and fomites
Part 6: A list of what to do where and when
(If you want to read only one of these installments, this would be the one)
Part 7: Testing and medications
Part 8: Vaccination and risks (in general) and risks of vaccination vs. COVID
Part 9: Morality of COVID (Section 1 of 2)
Part 10: Morality of COVID (Section 2 of 2)
Part 1:
How bad is COVID, really, and what to do with the new CDC recommendations?
I haven’t gotten COVID… yet. I know, it sounds like bragging. But, there are plenty of reasons for myself (and my wife) having avoided this sometimes horrible disease so far. If you are wondering, we DO NOT have freakishly potent immune systems – quite to the contrary. I will talk more about myself and why you should listen to me later.
To start, I want to recommend my favorite, consistently good sources of information and advice. These are very well-written, clear, and well-researched, and usually make a lot of sense:
1. Katelyn Jetelina from “Your Local Epidemiologist” <yourlocalepidemiologist.substack.com>
2. Leana S. Wen, M.D., Washington Post
3. Centers for Disease Control and Prevention (CDC), mostly for data and charts: https://covid.cdc.gov/covid-data-tracker/#datatracker-home
So, why AM I writing this? First, COVID is NOT going away. Why would it? It has done a great job infecting people. It’s not going to hang up the spikes any time soon (pun intended). In fact, as of the first week of August, 2024, we are experiencing a new summer spike of COVID infections, even higher than multiple prior spikes. COVID might go away eventually if there are much more effective, or universal coronavirus vaccines (at least for people willing to get vaccinated), or highly effective medications developed (for people willing to take them). So, we are stuck with COVID for a long time to come.
Second, there is a fundamental problem with understanding public information about COVID. You hear a lot from “public health” officials. However, what public health professionals and officials talk about is meant for government, businesses, and other organizations to issue policies and recommendations. These are the things that people get really upset about because of suspicion of errors and biases, difficulties of implementation, and so on.
KEY POINT:
How you manage your personal health is very different from how you should react to public health declarations. You are an individual, not “the public.”
To be clear, I have great respect for public health professionals, how much they care, and how difficult their jobs are. What they say is interesting and somewhat relevant to you, because someone with authority might suggest or make you do what they say. However, basically, to them, it’s not about YOU. It’s about GROUPS of people like you. Obviously, they don’t know you. But, you don't go to a public health official when you are sick, you go to a doctor, or another trained health professional. You will see more why that is important as I go on.
So, let’s dig into that idea by looking at the latest CDC recommendations (shortened, paraphrased) regarding isolation and testing for COVID infections – and actually, now, pretty much any upper respiratory infection (URI):
· Stay home when sick until your fever is gone for 24 hours AND your symptoms improve.
· What does “symptoms improving” mean? If you only have a mild cough or runny nose left and you feel pretty much OK.
· For 5 more days, use precautions, including using masks correctly, and taking tests before seeing vulnerable people.
Why should we still be concerned about COVID more than other URIs? Isn’t COVID pretty much like the flu? Spoiler alert: not even close. Here is a headline from the Wall Street Journal on 3-1-24: “It’s Official: We Can Pretty Much Treat Covid Like the Flu Now.” But, can we? Further down, the article states: “Let’s be clear. Covid-19 is not the flu. It still causes more serious illness and leads to more lasting effects.”
A couple of months ago, I read the following online: “While COVID deaths and hospitalizations are still higher than the flu, … the disease is no longer considered an emergency.” Guess what, I bet that if YOU get COVID and can barely breathe, you will think that it IS an emergency for YOU, even if it is NOT an emergency for a public health official. They act because there are a lot of people getting sick, not because YOU are sick.
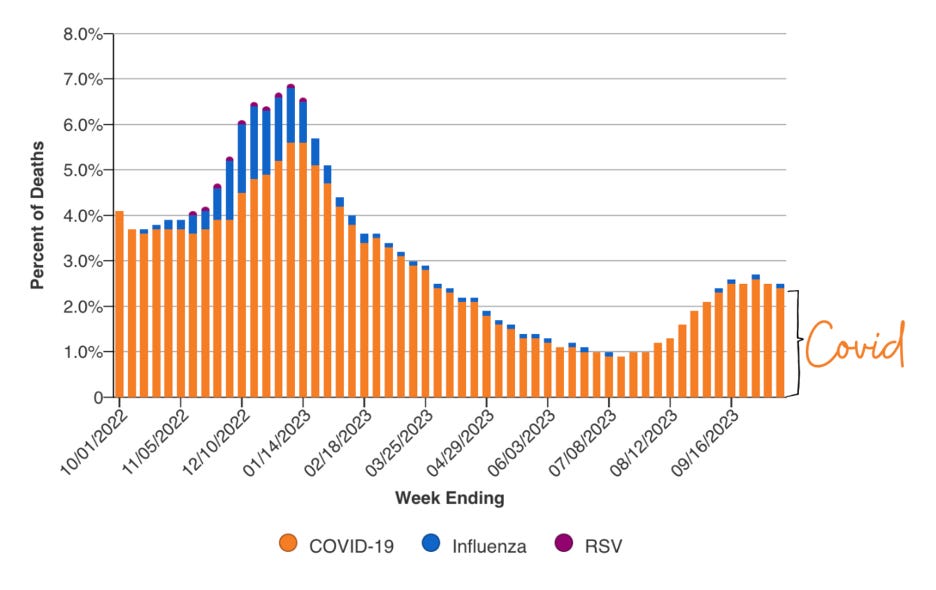
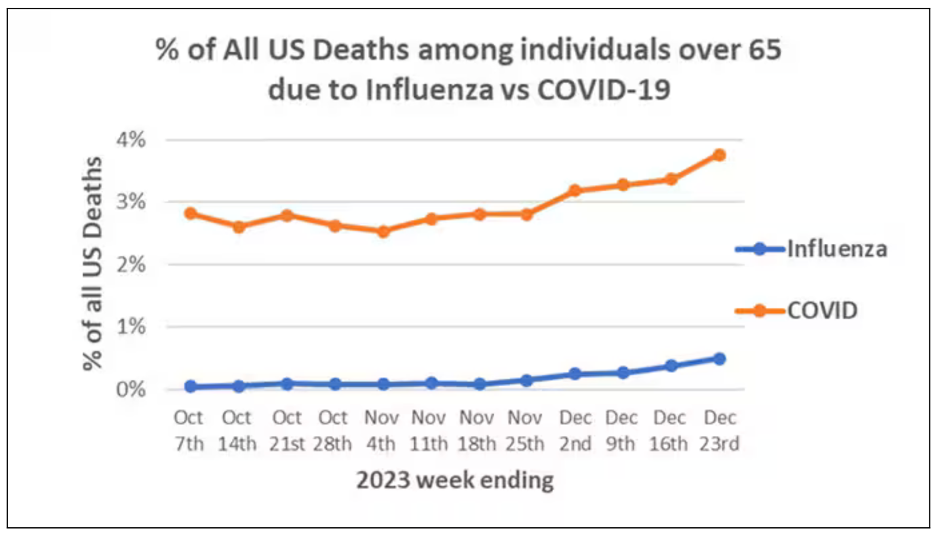
How much worse is COVID, really, than the flu? First, you should know that at the end of this past winter’s (2023-2024) surge, about 1.8% of ALL deaths in the US were from COVID! Look at the chart below from late 2022 to late 2023. Notice that the VAST majority of deaths from upper respiratory infections (URIs) were from COVID.
CDC data annotated by Katelyn Jetelina from Your Local Epidemiologist 10-31-23
CDC data printed by Katelyn Jetelina from “Your Local Epidemiologist” 1-11-24
OK, so, it’s not even close. Why does the CDC suggest that we treat COVID more or less like the flu? I think that they, and many others are pretty open about that. They’re simply convinced that the more complicated that recommendations are, the less likely you will follow them. I bet that you think that, too. I ALSO think that. So, they want recommendations that they THINK you MIGHT follow. However, this advice is meant for GROUPS. Again, you are not a GROUP.
One other point about a fallacy of thinking about COVID vs. flu: Let’s just assume, incorrectly, for the moment, that flu deaths and COVID deaths were comparable, as many have erroneously said. Even if that were true (again, it’s not even close), then up to twice as many people would be dying of upper respiratory infections. We should want to prevent deaths from both, not accept deaths from COVID because it supposedly isn’t any worse than the flu. You could get both.
My thoughts about the new CDC recommendations? You probably have already figured out that I do not feel 100% comfortable with them, given the consequences of you actually infecting someone with COVID because you are less careful than you could be. Maybe the next person to catch it from you will recover quickly and completely, but what if, say, the 20th person down the line is hospitalized or dies? No one, including you, will EVER know, but you would be responsible for a death (let alone long COVID), nonetheless. If that doesn't bother you, your and my values are not aligned. See Part 10 on COVID morality.
Let’s turn this around: how do you feel about one of your co-workers walking around, maybe or maybe not wearing their (N95?) mask properly, still coughing? Maybe you’re happy that YOU can do that, but what about them exposing you? What if YOU are immunocompromised or older, or have other medical conditions?
However, I will admit that there are some reasons and statistical evidence that the newest CDC recommendations (from spring, 2024) make some sense:
· Most infections are spread by pre-symptomatic or asymptomatic people, or in the first 3 days of symptoms.
· Some studies in US states and foreign countries found that after implementing a policy like this, transmission frequency didn’t change.
· Testing for COVID may not make much sense anymore until about 3 days into symptoms because of how many false negatives there are now.
Important point about testing: how fast it turns positive and how bright the line is makes a difference. Fast and bright means more likely you are more contagious.
· Lots of people don't know what virus they have anyway, so why not make the guidance the same for all of them? (Answer: because COVID is MANY TIMES worse than other URIs.)
Regarding those studies, the number of people included was not huge, bringing their conclusions into question. Also, once people are told that they can go out, I don't trust them to be careful with masks and to really try hard not to expose others.
So, what to do? It makes more sense to stay home after the 5 days until you test negative, if you can afford to wait. Infectiousness often runs out to 10 days or so. If you can’t afford to stay home, you CAN afford to be extra careful around others by wearing a mask, avoiding prolonged, personal contact with others and washing your hands when appropriate.